Non-Invasive Prenatal Paternity testing
Non-Invasive Prenatal Paternity testing
The test requires a blood sample from the mother and a buccal swab collection from the father.
Can I Get a Paternity Test While Pregnant?
Yes, you can get a paternity test while pregnant, and as early as 8 weeks. The test gives you an accurate paternity answer without any risk to you or the pregnancy – it’s completely safe.
How Prenatal Paternity Testing Works
Free-floating fetal DNA combines with the mother’s DNA by passing through the placenta into the mother’s bloodstream. The fetal DNA is isolated and analyzed during the testing process, and then compared to the possible father’s DNA profile.
Restrictions for Paternity Testing While Pregnant :
- A woman must be at least 8 weeks pregnant to test
- A prenatal paternity test cannot be performed for a woman expecting twins or multiples
- We cannot perform testing with two possible fathers who share a close biological relationship
DDC is one of the most trusted laboratories in the world, capable of delivering quality results to our most important client – you. Results are completely confidential, and your private genetic information is never shared with or sold to outside parties.
Fasting is not required prior to the test. Both the mother and the father must bring a valid photo identification document.
The test results will be available within ten days.
The test is carried out at the Elite Clinic upon registration for a consultation with Dr Deniss Sõritsa or Dr Andrei Sõritsa, available on Mondays, Tuesdays, Wednesdays, and Thursdays.
Please note that the test cannot be performed on the day preceding a public holiday.
Service providers
The test is carried out at the Elite Clinic upon registration for a consultation with Dr Deniss Sõritsa or Dr Andrei Sõritsa, available on Mondays, Tuesdays, Wednesdays, and Thursdays. Please note that the test cannot be performed on the day preceding a public holiday.


Price
| Service | Price |
|---|---|
Non-invasive prenatal Paternity Test Kindly note that the gynaecologist`s consultation fee and the ultrasound examination fee are not included in the price and will be charged separately. Additional test person: 300€ | 1650€ |
| Booking | |
|---|---|
Book Time |
The source of infection is another person infected with the papillomavirus. Human papillomavirus infection may cause changes in cells that may develop into precancerous conditions and cervical cancer.
Cell changes develop over a longer period of time. The process usually takes time and may take up to 10–25 years. Participating in the screening helps to detect possible cell changes and precancerous conditions in time, that these can be treated so actual cancer will not develop.
Cervical cancer is not hereditary. All women of all ages can develop cervical cancer. In Estonia, the prevalence and mortality of cervical cancer is one of the highest in Europe.
Why should you participate in the screening?
- Cervical cancer screening searches for precancerous conditions, which means that the screening enables to prevent cancer.
- Free and easily accessible: in Estonia, cervical cancer screening is free for women in the target group, including for the uninsured, and screening is performed in various health care facilities all over the country. By participating in the screening you demonstrate that you care about your health.
- It is important to participate in the screening even if you do not have any signs or symptoms. In case of early detection, it is possible to fully recover from the disease.
How to participate in cervical cancer screening?
You can participate in the screening in the following ways: .
- Schedule an appointment in Elite Clinic`s digital health booking system.
- Phone us and tell that you wish to book a screening appointment.
Who are invited to cervical cancer screening?
In Estonia, women aged 30–65 are invited to cervical cancer screening every five years. Screening tests are free for all insured and uninsured women who belong to the screening test target group for a given year. Women who have not been sexually active or whose last intercourse was many years ago are still invited to a screening, as it may take decades for the viral infection to develop into cancer.
Screening invitation
The Cancer Screening Registry will send a personal invitation to women in the target group.
Women whose year of birth is part of the screening target group and whose place of residence is the Republic of Estonia at the time of generating the screening invitation/referral are invited to a screening.
Invitations to screenings are sent electronically, using the notification service of eesti.ee. An e-invitation will be sent to persons in the screening target group whose eesti.ee email address has been redirected to their personal email address or entered in the population register.
If there is no data on the redirection of emails in the Cancer Screening Registry, a paper invitation will be sent to the address entered in the population register. If data in the population register is inaccurate, the invitation may not reach the recipient.
Colposcopy
Colposcopy is a medical procedure used to examine the cervix, vagina, and vulva for signs of disease. It involves using a special magnifying device called a colposcope to get a detailed view of these areas, allowing healthcare providers to identify any abnormal cells or conditions.
Insertion of intrauterine device
An intrauterine device (IUD) is a form of birth control that a healthcare provider inserts into your uterus.
To insert your intrauterine device, your healthcare provider will:
- Clean your cervix with an antibacterial solution
- Use a plastic insertion tube to guide the IUD through your vagina and cervix, and slide it into your uterus
- Use a slider, on the insertion tube, to push the device into your uterus
Your provider might advise you to take a pain management medication an hour before your scheduled IUD insertion.
An IUD insertion is usually a quick procedure you can have at a provider’s office. Many people will only experience mild discomfort, but others can experience more pain. Talk to your provider about any anxiety you may have regarding the procedure and ask about strategies they recommend to relieve any pain.
Before the insertion of the device, a gynaecologist appointment is required.
Kolposkoopia on oluline meetod emakakaelavähi ja vähieelsete seisundite avastamiseks, mille sagedaseks tekitajaks on inimese papilloomiviirus (HPV). Kolposkoopia abil on võimalik paremini tuvastada emakakaelas olevad muutused.
Uuring on ohutu ja valutu.
Kolposkoopilist uuringut ei saa teostada menstruatsiooni ajal. Uuring teostatakse günekoloogilises toolis sarnaselt günekoloogilisele läbivaatlusele. Uuring kestab 15–20 minutit.
Kusepõis peab olema tühi ja soovitav on hoiduda suguelust 24 tundi enne uuringut.
Kolposkoopia läbiviimiseks asetatakse tuppe vaginaalne peegel ning visualiseeritakse emakakael täies ulatuses. Vajaduse korral võetakse haigestunud piirkonnast väike koetükk ehk biopsia histoloogiliseks uuringuks.
Teenuseosutaja



Service providers
Service provider

Maie Väli
Endocrinologist
Service Provider

Mida on võimalik spermast analüüsi käigus kiiresti hinnata?
- spermatosoide hulka ehk kontsentratsiooni
- spermatosoidide liikuvust ja nende erinevaid kategooriaid: kiired progresseeruvad, aeglased-progresseeruvad, kohapeal liigutavad ja liikumatud
- spermatosoidide üldist välimust-ehitust – morfoloogiat: normaalsete vormide osakaalu, pea-, akrosoomi-, keskosa-, saba- ja arengudefektide osakaalu ja mitme defekti koosesinemise oskaalu ühe spermatosoidi kohta (teratozoidindeks)
- seemnevedeliku hulka, värvust, lõhna ja pH väärtust (happelisust-aluselisust), mikroobide ja muude rakuosiste esinemist – annavad teavet mehe sugunäärmete tööst ja suguteede olukorrast
- spermatosoidide kokkukleepumist ja selle määra (võib teatud juhtudel olla loomulikku viljastumist takistavaks teguriks)
- spermatosoidi membraani terviklikkuse hindamise juures on abiks test, mille abil hinnatakse spermatosoidide käitumist hüpoosmootses keskkonnas – terve membraaniga spermatosoidide sabad “tõmbuvad krussi” ja vigastatud membraaniga (N: surnud) spermatosoidide sabad jäävad sirgeks
- seisvate spermatosoidide suure osakaalu puhul saab spetsiaalse värvimisega teha kindlaks, kui suur osa neist on surnud, palju elus (teatud puhkudel võib spermatosoidi liikumatuse põhjuseks olla mingi saba või keskosa struktuurianomaalia, mis enamasti siis juba
geneetiline) – kehavälise viljastamise juures võimalik süstemeetodit kasutades elavaid, kuid liikumatuid spermatosoide kasutades munarakke edukalt viljastada ja järglane saada.
Mees peaks enne spermaanalüüsi jaoks materjali andmist eelnevalt 3-5 päeva seemnepurskest hoiduma. See annab selgema pildi tema seemnerakkude tootmisest ja viljastamise võimekusest (seemnerakkude hulk ja liikumine).
Mis vahe on üldspermaanalüüsil ja täisspermanalüüsil?
Üldspermanalüüsil hinnatakse ejakulaadis olevate seemnerakkude hulka ehk kontsentratsiooni, spermatosoidide liikuvust ja nende erinevaid kategooriaid: kiired progresseeruvad, aeglased-progresseeruvad, kohapeal liigutavad ja liikumatud, spermatosoidide üldist välimust-ehitust – morfoloogiat: normaalsete vormide osakaalu, pea-, akrosoomi-, keskosa-, saba- ja arengudefektide osakaalu ja mitme defekti esinemise oskaalu ühe spermatosoidi kohta (teratozoidindeks), seemnevedeliku hulka, värvust, lõhna ja pH väärtust (happelisust-aluselisust), mikroobide ja muude rakuosiste esinemist – annavad teavet mehe sugunäärmete tööst ja suguteede olukorrast, spermatosoidide kokkukleepumist ja selle määra, seisvate spermatosidide suure osakaalu puhul saab spetsiaalse värvimisega teha kindlaks, kui suur osa neist on surnud, palju elus.
Täisspermaanalüüsi korral teostatakse lisaks üldspermaanalüüsi korral teostatavale:
- funktsionaalsed testid (edasiliikumiskiiruse hindamise ehk penetratsioonitest, antikehadega seostumise test, hüpoosmootne test)
- liikuvate seemnerakkude eraldamine kõigi ejakulaadis olevate seemnerakkude hulgast – analoogselt loomulikul teel viljastamisega ja nende elusate-liikuvate seemnerakkude viljakusnäitajate (kontsentratsioon, liikumisaktiivsus, morfoloogia) määramine.
See annab palju selgema ettekujutuse loomulikul teel viljastamise võimaluse kohta.
Samuti on see viljakusravi vajaduse puhul määravaks osaks millise meetodi kasutamine (emakasisene viljastamine ehk IUI, IVF, ICSI) võiks kõige tõenäolisemalt positiivse tulemuse anda.Spermaanalüüsi teostab bioloog Andre Taimalu.
| Booking | |
|---|---|
Broneeri iseteeninduses |
Üldspermanalüüsil hinnatakse:
- seemnevedeliku hulka, värvust, lõhna ja pH väärtust (happelisust-aluselisust),
- ejakulaadis olevate seemnerakkude hulka ehk kontsentratsiooni,
- spermatosoidide liikuvust ja nende erinevaid kategooriaid: kiired progresseeruvad, aeglased-progresseeruvad, kohapeal liigutavad ja liikumatud,
- spermatosoidide üldist välimust-ehitust – morfoloogiat: normaalsete vormide osakaalu, pea-, akrosoomi-, keskosa-, saba- ja arengudefektide osakaalu ja mitme defekti esinemise oskaalu ühe spermatosoidi kohta (teratozoidindeks),
- mikroobide ja muude rakuosiste esinemist – annavad teavet mehe sugunäärmete tööst ja suguteede olukorrast,
- spermatosoidide kokkukleepumist ja selle määra,
- seisvate spermatosidide suure osakaalu puhul saab spetsiaalse värvimisega teha kindlaks, kui suur osa neist on surnud, palju elus.
Service Provider
Service Provider
Service Provider
Service Provider
PSA määramist kasutatakse eesnäärmevähi riski varajaseks avastamiseks ja ravi efektiivsuse hindamiseks. PSA-testi tegemiseks pöördu uroloogi konsultatsioonile.
Alates 50. eluaastast on soovitatav teha kord aastas PSA-test. Kui aga lähisugulastel on diagnoositud eesnäärme- või rinnavähki, on esmane kontroll soovitatud juba 45aastaselt.
PSA määramiseks on vajalik vereanalüüsi andmine.
Service provider
Service provider

Kaja Julge
Allergy specialist
Personaalne toitumiskava
Toitumisnõustamiselt saate kaasa personaalse toitumiskava ja nõuanded, mis on koostatud võttes arvesse teie vanust, pikkust, kaalu, tervislikku seisundit, füüsilist koormust ning eesmärke.
Toitumisspetsialist aitab:
- Raseduseelne kaalu langetamine, tõstmine või kehakaalu stabiliseerimine
- Rasedusaegne loote arengut toetav kehakaalu kontrollimine
- Kehakaalu kontroll rinnaga toitmise ajal
- Toitumine taimetoitlastele
- Toitumine kuni 50-aastastele (kehakaalu langetamine, tõstmine ja hoidmine)
- Toitumine üle 50-aastastele ja muud eapõhised toitumissoovitused
- Toitumine/dieet enne maovähendusoperatsiooni (laparoskoopiline maost möödajuhtiv operatsioon, laparoskoopiline vertikaalne maoresektsioon, laparoskoopiline maopael)
- Toitumine pärast maovähendusoperatsiooni
- Toitumine/dieet muude seedeorganite operatsioonide puhul
- Toitumine/dieet südame-veresoonkonna, neerude, endrokrinoloogiliste (suhkruhaigus, kilpnääre), ainevahetushäirete (podagra, rasvumine), liigeste, hingamisteede, neuroloogiliste haiguste korral
- Toitumine/dieet traumade korral
- Toitumine/dieet põletushaiguste korral
- Lisaks toitumisele pakume personaalset treeningnõustamist vastavalt teie soovidele, eesmärkidele ning tervislikule seisundile treeninguks kas spordiklubis või õues.
Teenuseosutaja

Artur Minenko
Nutritionist
Toitumisspetsialisti esmane konsultatsioon
Esmasel konsultatsioonil soovime teie kohta võimalikult palju teada saada, et kujundada toitumiskava just teile sobivaks – teie elustiil, sportlik aktiivsus, toitumisharjumused ning mis peamine – tervislik seisund ja eesmärgid. Varuge aega umbes tund. Palume teil täita küsimustiku, mõõdame teie kehakaalu, määrame kehamassiindeksi ning vajadusel mõõdame vererõhku ja pulssi. Räägime teie muredest ja eesmärkidest.
Koostame teile toitumiskava, milles on toodud teie päevane valkude, rasvade ja süsivesikute vajadus toidukordade kaupa. Kavas on lihtsalt ja arusaadavalt lahti seletatud, kui palju makrotoitaineid erinevad toiduained sisaldavad – milliseid toite neist endale valmistate, valite ise.
Toitumisspetsialisti teenus sisaldab ühekordset ühist toidupoe külastamist, et välja selgitada, millised toiduained/valmistoitude valikud tema tavapärases toidupoes on antud inimese jaoks kõige sobilikumad. Ühise poekülastuse eesmärgiks on aidata inimesel kaubavalikus orienteeruda, õpetada teda mõistma toitumisalast teavet/koostisosi toiduainete ja valmistoitude pakenditel, tagada toidukorvi tasakaalustatuse, viia kurssi end tervislike valikutega.
Ühine valikute tegemine aitab ka inimesi, kes teatud haiguste tõttu peavad toidusedelis tegema muudatusi ja kohanema uue eluviisiga.
Toitumisspetsialist selgitab lühidalt ka poodide tavapärast ülesehitust ja nn lõkse, et igapäevaste sisseostude tegija saaks kätte just need kaubad, mille järele ta on tulnud ja loobuks nendest, mida ei vaja, kuid mida poed väljakutsuvalt presenteerivad.
Toitumisspetsialist aitab välja tulla rutiinist ja näidata ka alternatiivseid valikuid ja juhendada, kuidas neid saaks igapäevases menüüs rakendada.
Täiendav toidupoe külastus koos toitumisspetsialistiga maksab 25 eurot.
Mis edasi?
Toitumiskava saate kätte järgmisel visiidil, mil ootame teid tagasi meie kabinetti, kus toitumisspetsialist seletab kava iga punkti lahti ning vastab tekkinud küsimustele. Kava järgimisega saate algust teha kohe.
Et uue elustiiliga harjumine võimalikult kiirelt ja kergelt läheks, pakume lisaks toitumiskavale võimalust saata iga päeva lõpus või ülepäeviti oma toitumispäevikuid. Toitumisspetsialist vaatab päeviku üle ning annab tagasisidet, milliseid makrotoitaineid sõite sel päeval liiga palju, milliseid liiga vähe, võttes arvesse teie füüsilist aktiivsust.
Toitumispäevikud on saadaval 10-päevaste pakettidena ning neid võib kasutada piiramatu aja jooksul – just nii kaua, kuni tunnete end üksi täiesti kindlalt. Toitumiskavaga on kaasas esimene 10-päevane päevikute pakett. Toitumispäevikuid saab saata e-maili või Facebooki kaudu.
Teame, et uuega harjumine ning soovitud eesmärkide saavutamine võtab aega – seepärast oleme teie jaoks olemas ka edaspidi. Koostöös endokrinoloogiga aitame leida vastused tekkinud küsimustele.
Esimene visiit
- räägime teie toitumisest (harjumused, kogused jne)
- täidame ankeedi teie andmetega (vanus, kaal, pikkus, vajadusel vererõhk ning kehamassiindeks)
- vaatleme teie tavapäraseid toiduaegu, et saaksime toitumiskava koostamisel neid arvesse võtta
- saame ülevaate teie liikumisharjumustest ning füüsilisest koormusest
- hindame makrotoitainete (valkude, rasvade, süsivesikute) tasakaalu teie tavapärases toitumises
- juhime tähelepanu ning selgitame puudujääke teie tavapärases toitumises
- anname nõuandeid, mida saate oma toitumises ise kohe muuta, juba enne toitumiskava kättesaamist
- vajadusel anname nimekirja soovituslikest vere- ja uriinianalüüsidest (vt allpool), mis aitavad efektiivsema toitumiskava koostamisel
Teine visiit
- koostame teile personaalse toitumiskava
- räägime toitumiskava üksikasjalikult lahti ning anname lisasoovitusi toitumiseks ning kehaliseks aktiivsuseks
- vastame küsimustele
- teeme teist foto progressi jälgimiseks (nõusolekul)
- anname toitumiskavaga kaasa toitumispäeviku faili 10 päevaks
- anname ülevaate analüüside tulemustest
- anname tagasisidet meile saadetud toitumispäevikute kohta e-maili, Facebooki või telefoni teel 10 päeva jooksul
- palume toitumispäevikud saata e-maili või Facebooki teel iga päeva õhtul või ülepäeviti, et oleks võimalik aegsasti tagasisidet anda – osutada vigadele toitumises ning pakkuda välja paremaid alternatiive
10 järgmist toitumispäevikut
Toitumiskavaga kaasas olevale 10 toitumispäevikule lisaks pakume 10 toitumispäeviku komplekti (10 päevaks). Toitumispäevikute täitmine ning analüüsimine aitab mõista tasakaalustatud toitumise põhimõtteid.
- jälgime teie igapäevast toitumist ning vajadusel teeme toitumiskavasse muudatusi (kui kaal pikema ajaperioodi vältel ei muutu)
- selgitame teile teie keha toitainete vajadust hetkel
- anname tagasisidet meile saadetud toitumispäevikute kohta e-maili, Facebooki või telefoni teel 10 päeva jooksul. Palume toitumispäevikud meile saata e-maili või Facebooki teel iga päeva õhtul või ülepäeviti, et saaksime teile aegsasti tagasisidet anda – osutada vigadele toitumises ning pakkuda välja paremaid alternatiive.
Analüüsid
- TSH
- Prolaktiin
- Kortisool
- Üldtestosteroon
- Estradiool (E2, Estradiol)
- PTH
- Insuliin, glükoos (GTT)
- AST ja ALT-maks
- LDL
- HDL
- Triglütseriidid TG – (Triglycerides)
- Kreatinin (Creatinine)
- Üldvereanalüüs
- Ülduriinianalüüs
Alati võite pöörduda meie poole treeninguid puudutavates küsimustes (kas vastuvõtul, e-maili, Facebooki või telefoni teel). Soovi korral koostame treeningkava spordiklubis või vabas õhus treenimiseks, võttes arvesse teie tervislikku seisundit ja eesmärke.
| Booking | |
|---|---|
Broneeri iseteeninduses |
Vaata lisaks
Method
In vitro activation of ovaries – methodology, used on women with premature ovarian failure where the growth of primary and secondary follicles are stimulated and as a result of that, these women are able to get ripe oocytes with IVF (in vitro fertilization) and after fertilization become pregnant and have a baby. There have been cases of natural conception after IVA.
Activation occurs in laboratory conditions after the removal of ovarian tissue during laparoscopy. The studies showed that when surgically removed ovarian tissue were split, then the ovarian growth pathways (Hippo signal route) activated and as a result of that the growth of “sleeping ” oocytes occurred.
Ovarian activation surgical method was presented for the first time by Japanese investigator Kazuhiro Kawamura in year 2010.
Following the use of this method, the world’s first child was born in 2013.
Since then, several countries have started to use this method (Japan, China, Spain, Poland, Mexico, Russia, India). Several children have already been born as a result of this method and there are different variations of the methodology in use.
The TIME magazine (USA) has nominated this method as one of the ten best medical achievements in the world.
Indications for ovarian activation
- Different causes for ovarian failure. Decreased ovarian reserve.
- The absence of oocytes in IVF program.
- Empty follicles syndrome when in IVF program there has not been any egg cells to be extracted.
- If follicles do not grow during stimulation despite the use of high gonadotropins medications.
- If the ovaries do not work after a trauma due to surgery.
- High FSH levels (range 30-150 UI/L) and low AMH levels (zero or close to zero).
How IVA is performed at Elite Clinic?
Dr. Andrei Sõritsa will perform the necessary examinations during the consultation, assess the possibility of the operation and discuss the expected effect and risks of IVA.
Foreign patients can send a description of their problem, hormone test results (FSH, E2 and AMH) and scan report (size and structure of the ovaries, size of all follicles, size and structure of the uterus, endometrium thickness) by e-mail: andrei@elitekliinik.ee.
In some cases, you might be asked to start a hormonal preparation already before the operation. You will be offered the time for laparoscopic surgery. You need to be healthy for the time of surgery. You should not have diseases that increase the risk of the surgery.
For the operation you will come in the morning to the Elite Clinic, thereafter the surgery will be performed and in the evening you can leave the clinic and drive home (you are allowed to fly the day after the operation).
The operation is performed under general anaesthesia and will take approximately 1,5 hours.
During the operation, the doctor removes a piece of the ovarian tissue size about up to 2 x 2 cm, splits it in IVF solution and puts small ovarian pieces sized about 1x1x1 mm with catheter into another ovary and under the peritoneum near the ovary and stitches it together.
After the operation, it is recommended to rest for 3 days at home. If necessary, you can ask the doctor for a sick leave verification letter.
Efficiency of the operation
The current world studies show that approximately 50% of women who has undertaken follicle activation surgery, indicate the activation of the ovaries which is sufficient for the formation of oocytes, for fertilization and embryo transfer. Some women start to have menstruations again.
Unfortunately, before the operation, there is no way to predict how many “sleeping” follicles there are left in woman’s ovaries and how they will react to the activation.
The IVA method makes it possible to obtain oocytes from women who have stopped the oocytes production naturally. However, this method cannot improve the quality of the egg cells, which means that this method is most suitable for women aged up to 41, especially aged up to 35 or when the menopause length is less than 4 years.
Even after the age of 41 years, the IVA method gives a higher likelihood of obtaining oocytes, but the quality of the egg cells still remains consistent with age. The quality of the egg cells drops dramatically after 43 years of age
When to expect an IVA effect?
Based on the condition of the patient before the surgery, the doctor will give you after surgery a timeline to start with ovarian stimulation and IVF procedure either immediately after surgery, a month later or once AMH rises and FSH lowers, which can take up to 6 months.
It should be taken into account, that initially follicles need to be grown using high doses of medications, then retrieve the oocytes, to fertilize them and freeze embryos. Most likely such procedure needs to be performed repeatedly for as long as there are good embryos for transfer. Only then the frozen embryos transfer can be planned. If they wish, foreign patients can have an IVF procedure in their home country.
How long can it take to act?
No precise data are available at the moment. The best effect of ovarian activation is expected in the first year after surgery.
Analyses required for laparoscopic surgery
- Bloodgroup and Rh factor,
- PAP test (valid for 24 months),
- T.pallidum Ab, HIV, HBsAg, HBcAb, anti-HCV, full blood count; Gonorrhoea, Trichomonas, Chlamydia (valid for 3 months).
The risks of laparoscopic surgery
The risk of operation is below 0.3%. You can read the description of laparoscopic surgery on the Elite Clinic’s website.
Dr. Andrei Sõritsa is an experienced surgeon who has performed over 1000 different laparoscopic surgeries during his lifetime.
Risks of IVA
There are no reported complications regarding IVA. There is no evidence that IVA raises the risk of cancer in women. But today, less than a thousand such procedures have been carried out in the world and it is too early to draw definitive conclusions on its effectiveness and potential risks.
Price of IVA
| Service | Price |
|---|---|
IVA test (with Estonian Health Insurance) The price does not include analyses nor consultations. | 3700 € |
IVA test (without Estonian Health Insurance) The price does not include analyses nor consultations. | 4800 € |
If ovarian tissue is frozen during the procedure, an additional €490 will be charged for freezing and storage (for the first 3 months). Further storage costs €1 per day.
In order to assess your indications and contraindications for surgery, as well as to estimate the likelihood of becoming pregnant after surgery, please fill in the form, attach your (and your husband’s) the results, the scan report of the uterus and ovaries, and book a Skype/FaceTime, WhatApp or Viber consultation. The price for consultation is 150/170 EUR.
Could this method be effective in your case? You can make an inquiry by phoning to Dr. Andrei Sõritsa on +372 5052295.
| Booking | |
|---|---|
Schedule your appointment online |
Who Might Consider Freezing Their Eggs?
Egg freezing can be a valuable option for women who wish to preserve their fertility for various personal, medical, or ethical reasons.
- Women who wish or need to delay childbearing. Women who want to postpone having children due to education, career, or personal reasons may benefit from freezing their eggs at a younger age. As fertility naturally declines with age, freezing eggs during peak fertility years offers the best chance for future pregnancy. Unlike eggs, the uterus does not age significantly, and women can often carry a pregnancy successfully even in their 40s or early 50s. Importantly, the quality of frozen eggs does not decrease over time.
- Women diagnosed with cancer. Cancer treatments such as surgery, chemotherapy, or radiation can damage or destroy eggs, leading to infertility. Freezing eggs before treatment allows the opportunity to preserve fertility. While some women may still have viable eggs post-treatment, fertility preservation is highly individual and depends on age, cancer type, and treatment plan.
- Women with ethical or religious concerns about embryo freezing. Some women or couples prefer not to freeze embryos due to religious or moral beliefs. During standard IVF treatment, there may be surplus embryos that are not used immediately, raising ethical concerns about their storage or disposal. In these cases, fertilizing only the number of eggs needed for the IVF cycle and freezing the remaining unfertilized eggs may be a more acceptable solution.
- Women with a family history of early menopause. Some forms of early menopause can be hereditary. If there is a family history, freezing eggs early can preserve fertility before egg reserves are depleted.
How Are Eggs Frozen?
Unlike sperm or embryos, which are relatively easy to freeze, the egg is the largest cell in the human body and contains a high amount of water. This makes it more vulnerable to damage from ice crystal formation during freezing. To prevent this, the water in the egg is replaced with a cryoprotectant (an antifreeze-like substance), which protects the cell during freezing.
Because the shell of the egg becomes harder after freezing, fertilization later requires intracytoplasmic sperm injection (ICSI), where a single sperm is injected directly into the egg.
There are two main methods of egg freezing:
- Slow freezing
- Vitrification (rapid freezing) – now the preferred and more effective method.
What Is the Egg Freezing Process Like for the Patient?
Egg freezing involves a process similar to standard IVF. The only difference is that after the egg retrieval, the eggs are frozen instead of being fertilized right away.
The overall process takes around 4 to 6 weeks and includes:
- 2–4 weeks of hormone injections and possibly birth control pills to temporarily suppress natural hormones.
- 10–14 days of hormone stimulation to encourage multiple eggs to mature.
When the eggs are ready, they are retrieved using a needle guided by ultrasound through the vaginal wall. This is done under general anesthesia.
The eggs are then immediately frozen. When the woman is ready to attempt pregnancy — potentially years later — the eggs are thawed, fertilized with sperm, and the resulting embryos are transferred into the uterus.
How Long Can Frozen Eggs Be Stored?
Scientific studies confirm that long-term storage does not reduce the quality of frozen eggs.
In Estonia, only licensed fertility clinics may freeze and store eggs. The law does not currently limit the length of time eggs may be kept frozen.
How Many Eggs Should Be Frozen to Increase the Chances of Future Pregnancy?
For women under 38, typical expectations are:
- 75% of frozen eggs survive the thawing process
- 75% of thawed eggs fertilize successfully
This means that from 10 frozen eggs, around 7 will survive thawing, 5–6 may fertilize, and several embryos may develop. Usually, 1–2 embryos are transferred per cycle.
To maximize the chance of pregnancy, it’s recommended to freeze around 10 eggs per intended pregnancy attempt. Most women under 38 are able to retrieve 10–15 eggs in one cycle.
How Successful Is Egg Freezing?
According to statistics, around 65% of women who use their frozen eggs later go on to have a baby. (Source: fertilitypreservation.org’s calculator for pregnancy likelihood after egg freezing and thawing.)
Please note: Elite Clinic cannot be held responsible in cases where thawed eggs do not survive, fertilization is unsuccessful, embryo development is abnormal, or pregnancy does not occur.
What If a Woman Is Over 38 When Freezing Her Eggs?
The chances of pregnancy depend on the age at the time of egg freezing, not the age when the eggs are used.
Women older than 38 may have lower success rates, and it is not yet fully known whether eggs from women over 40 respond to freezing and thawing in the same way as younger eggs.
Is Egg Freezing Safe?
Yes. Over 10,000 babies worldwide have been born from frozen eggs. The largest published study, involving 900 children born from frozen eggs, found no increase in birth defects compared to the general population. There were also no increased risks of chromosomal abnormalities compared to embryos from fresh eggs.
A 2014 study also confirmed that pregnancy-related complications do not increase due to egg freezing.
Globally, over 300,000 children have been born from frozen embryos (mostly using slow freezing methods), without an increase in birth defects. However, ongoing studies continue to monitor long-term outcomes to ensure safety.
Price
| Service | Price |
|---|---|
Oocyte Cryopreservation (Tervisekassa kindlustuse olemasolul) | 1570 € |
Oocyte Cryopreservation (Tervisekassa kindlustuseta patsientidele) | 1930 € |
| Booking | |
|---|---|
Schedule your appointment online |
Service providers:
Further reading
Unlike traditional transfer media, embryo glue contains high concentrations of hyaluronan, a natural substance found in the female reproductive tract. Its goal is to improve the bonding between the embryo and the uterine lining during implantation.
Service Providers
| Service | Price |
|---|---|
EmbryoGlue | 340€ |
More information on the Vitrolife website
How does it work?
Your genes regulate the exact time when embryo implantation can take place.
The beREADY test analyses 67 marker genes that reflect the readiness of your uterus for embryo implantation.
The beREADY test is like insurance to guarantee that embryo(s) are transferred at an optimal time.
If your Window Of Implantation (WOI) is shifted and a second test is needed, it’s free!
Who should use beRedy test?
We believe that every woman considering IVF procedure can benefit from the personalised treatment plan that beREADY offers. It should always be done before valuable embryo(s) are transferred. The test is designed for all women, whether using their own or donated embryos. And suitable for both type of cycle – Hormone Replacement Therapy (HRT) or natural cycle.
Avoiding the issues caused by the displaced Window Of Implantation (WOI) with personalised IVF plan gives you a higher chance of getting pregnant with fewer attempts, saving you time and resources. Personalised approach is beneficial in all cases, not only if you have limited number of embryos or you have had multiple failed attempts.
What does the beReady test show?
The beREADY test measures maturity level of your endometrium for successful embryo implantation. The test results are reported in three main categories.The endometrium may be:
- RECEPTIVE (optimal readiness for embryo transfer)
- PRE-RECEPTIVE (the tissue needs extra time to mature)
- POST-RECEPTIVE (receptive period is over)
Based on the results, practical recommendations are provided for your doctor. More specifically, the detected receptivity is expressed as a score on the receptometer. A few samples of possible scenarios:
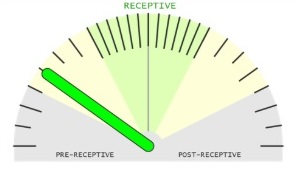
The sample is pre-receptive. It is not perfect time for day 5 embryo transferring. We recommend to repeat the test 24 hours later in the next cycle.The new test is highly recommended to confirm that your optimal WOI is achieved.
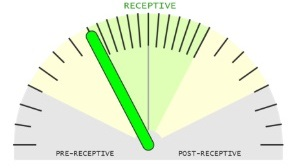
The sample is receptive but the optimal WOI is achieved in 12-24 h. No need to repeat the test.
We recommend to transfer the embryo 12-24 hours later.
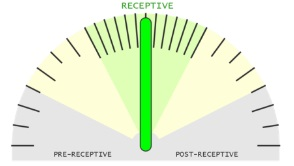
The sample is receptive. It is the perfect time for day 5 embryo transferring during the next cycle.
No changes are needed in your treatment plan.
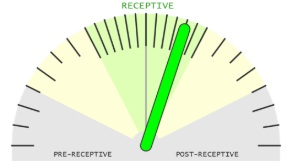
The sample is receptive but endometrial tissue maturation has been quicker and there is a risk that embryo implantation won’t take place. No need to repeat the test. We recommend to transfer the embryo 12 hours earlier.
Service providers
Price
| Service | Price |
|---|---|
Test for endometrial receptivity – beREADY + consultation`s fee, biopsy, histology, ultrasound investigation | 550 € |
| Booking | |
|---|---|
Schedule your appointment online |
Fertility test is recommended for women
- aged 30-35 years, who has yet not given birth
- aged 35-40 years, if it’s over 10 years from the last delivery
- 35-40 years of age, if pregnancy does not occur within one year of regular sexual intercourse
- those women who have had ovarian surgery (endometriosis, tumor)
- over the age of 30 years, if periods are irregular (fluctuations over 5 days)
- over the age of 30, if painkillers are required because of abdominal pain during every menstrual period
What is estimated during the test?
Taking into consideration the blood markers and ultrasound examination, ovarian reserve and fertility prospect is assessed.
What is the right time to have the test done?
During 3rd-5th day of a menstruation cycle. The first day of menstruation is considered day 1 of the cycle.
When to book the time for the test?
When the period starts, please call to Elite Clinic on +372 7409 930 to book an appointment time with doctor Andrei Sõritsa.
If there are no available times, please ask to speak to doctor Andrei Sõritsa himself to arrange additional appointment time.
What is important to know before the appointment?
- The appointment must take place in the morning prior to 12:30 pm and please take into consideration that performing the test takes about 40 minutes
- you need to come to the appointment in the morning fasting as well as without drinking
- for at least six weeks prior to the appointment do not use any hormonal medications, vitamins, food supplements or contraceptives
- 3 days prior to the appointment not to have sexual intercourse
- 6 weeks prior to the appointment do not visit a hot climate countries (except if you live there permanently)
- 6 weeks prior to the appointment do not go for an abdominal nor back massage, acupuncture, leach treatment, extra sensory or physiotherapy
Would the partner/ husband need to attend the appointment as well?
No. Analyses for a man are recommended if the woman does not become pregnant within one year of regular sexual activity without contraceptives.
Which questions could be answered?
- Is the ovarian reserve normal?
- What is the prognosis in terms of 5 years period to conceive a child?
- Whether there are tumors / endometriosis and their significance for conceiving a child?
- Whether it makes sense to preserve ones fertility, to freeze oocytes / embryos for the future?
- How much time one has in aspect of deciding when to have a child?
- Whether there is a need for medicament / surgical or artificial insemination?
- Whether there is a need for additional tests?
Dr. Andrei Sõritsa has 30 years of experience with the research and treatment with childless families. With his help thousands of children have been born after laparoscopy / hysteroscopy surgery, medicament therapy and artificial insemination.
How fast can I get an answer?
A written reply will be sent to a client’s e-mail address within 4-5 weeks. Additionally Dr. Andrei Sõritsa will call you and explain the results.
What is included in the test?
Included are vaginal examination, KOH test, BMI, blood counts, AMH, FSH, E 2, TNF, Ca 125, LH, ultrasound, AFC.
Price
| Service | Price |
|---|---|
Fertility assessment test + ultrasound investigation`s fee + gynaecologist`s consultation fee. | 330 € |
| Booking | |
|---|---|
Schedule your appointment online |
The main indications of venous thromboembolism genetic test are:
- commencing a hormonal contraception or hormone replacement therapy in a woman at risk group (patient or her close family has a history of thrombotic diseases, there is known existence of pro thrombophilic gene in the family)
- several unsuccessful artificial fertilization (IVF) attempts
- occurrence of venous thrombosis during pregnancy or woman taking oral contraceptives
- prenatal complications (recurrent miscarriages, pre-eclampsia or miscarriage)
- family history of venous thrombosis
- presence of pro venous thromboembolism gene in the family
- venous thrombosis <50 years of age
- heart attack on <50-year old woman who smoke
Venous thromboembolism (VTE) includes a deep vein thrombosis and pulmonary embolism.
Venous thromboembolism often occurs when several risk factors (genetic and acquired during life) occur simultaneously.
The most important acquired risk factors are considered to be major surgery and trauma. Moderate risk factors are considered to be pregnancy, taking birth control or HRT tablets, puerperium and tumors. Minor risk factors are considered to be immobilization/ immobilization of a limb in a forced position or paralysis due to prolonged air travel or other reasons.
Congenital or genetic factors which contribute to formation of venous thromboembolism are a mutation in Factor V Leiden, prothrombin G20210A mutation of the MTHFR gene and the C677T and A1298C mutations.
Table 1. Overview of genetic risk factors of venous thromboembolism:
| Genetic marker | Frequency | Risk |
|---|---|---|
| Faktor V Leiden | ~ 2.7% in Europe (0 – 7% depending on area), 3% in Estonia | Heterozygotes have 3-7 times greater risk of having VTE, homozygotes 50-100 times greater risk of VTE |
| Prothrombin G20210A | 1 – 8% in Europe, 3.3% in Estonia | 2-5 times greater risk of VTE heterozygotes, approximately 10-fold increased risk for homozygotes |
| MTHFR C677T | ~ 35% of Europeans are heterozygotes, homozygotes 12% | 2 to 3 times higher risk of VTE for homozygotes |
| MTHFR A1298C | 9-20% in all major ethnic groups | increased risk of VTE for heterozygotes if occurs with the heterozygous C677T mutation |
In case of existence of higher congenital VTE risks the following precautions should be subjected:
- Opt instead for hormonal contraceptives to prevent pregnancy by another means
- Consult with a doctor about hormone replacement therapy tactics with menopause
- Consult with a physician before operation regarding taking blood thinning medications
- Consult with a doctor if it is necessary to take blood-thinning medications during pregnancy and postpartum period
- Quit smoking
- Regular exercise to stimulate the blood flow and loose excessive weight
- During long trips to drink enough water and if possible, to move around in the meantime
With presence of genetic risk factors a medical consultation with skilled physician is needed to evaluate the risk of thrombosis and to assess the need for preventive treatment. It might be recommend for other members of the family to have a genetic counseling as well and to have the test in regard with present genetic changes.
| Service | Price |
|---|---|
Venous thromboembolism genetic risk assessment test + consultation with gynecologist and ultrasound | 600€ |
The results will be ready within 5-7 working day.
| Booking | |
|---|---|
Schedule your appointment online |